
Received my test results yesterday evening and finally hit ND (0.000%) after 3 years and 9 months.
Results of all tests since diagnosis:
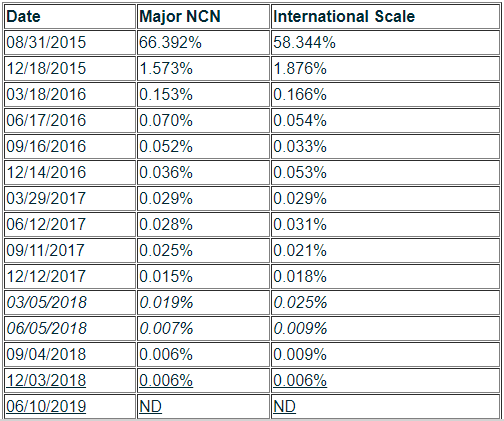
I want to highlight two area in the above chart, the first is in italics from 03/05/2018 through 06/05/2018. There was a slight bump up during this period and then a large drop (MMR to CMR) afterwards, the reason for this may have been due to an experiment my doctor and I tried. I stopped taking the experimental medication after the drop to CMR (due to side effects) and stayed stable at CMR for the next two testing cycles.
The next change is underlined in the chart above dated 12/03/2018 through 06/10/2019. After the 12/03 test I decided to go back to trying the experimental medication once again and did so for about two months during that window and the result was Non-Detectable. A few notes about this six month time period:
- My daughter was put in preschool during this time and was always getting sick which of course resulted in me becoming sick. I missed a lot of doses of medicine during those sick periods and also missed my dose the night before my blood test (forgot). I would say that overall, I likely missed about 20 doses during that time.
- I took the experimental medication around the March and April time frames and stopped taking it once again due to the side effects.
Drug Details
Medication: Misoprostol
Dose: 200 mcg
Availability: Prescription only (yes, it is and has been widely available for some time)
Details of when and how much I was taking and the side effects:
03/05/2018 through 06/05/2018 (began in February, ended in April)
1 times daily, 4 x 200 mcg at the same time as taking Imatinib dose (nightly, before bed).
12/03/2018 through 06/10/2019 (began in March, ended in April)
1 times daily, 8 x 200 mcg at the same time as taking Imatinib dose (nightly, before bed).
The typical dosage is to take one 200 mcg tablet (if you can call it that) every four hours. This is the standard dosage for people with ulcer problems. This medication is also used for abortions (in a higher does, which happens to be 1600 mcg which I was taking later on). Since I was not taking the medicine for ulcers, I decided to take the four doses (later eight) all at the same time as my Imatinib to increase the chance of it working.
Side effects:
Serious bouts of diarrhea (far more serious than with Imatinib). I eventually stopped taking it on nights before I had to work the next day and only took the Misoprostol if I knew I was going to be home the next day.
Bouts of dizziness. I am not 100% certain this was from the Misoprostol or the blood pressure medication I was also taking at the same time. The blood pressure medication (Losartan - HCTZ 50-12.5 mg) does have an interaction with Imatinib and I stopped taking it around the same time as I stopped taking the Misoprostol. I intend to take the Misoprostol again in the future and will update with any results.
So why Misoprostol?
It all began almost two years ago when I stumbled on an article (https://www.news-medical.net/news/20170926/Existing-drugs-may-be-able-to...) which made mention of two drugs which were currently available possibly being used to cure CML by eradicating the CML stem cells. I investigated the two medications and found Misoprostol to be the safer of the two. I inquired the possibility of testing this out with my Oncologist and he prescribed three months worth of the medication to me.
https://www.ncbi.nlm.nih.gov/pubmed/28844837
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5678929/
Now, there is no guarantee that this works, maybe my test results were just pure chance, maybe not, but after having been stuck at MMR for such a long time and reaching CMR (and DMR) after taking the Misoprostol, well, a sample size of one is not going to cut it so thought the best course of action would be to share these results with others. I do not know if your doctor will be as willing to try this as mine was and prescribe a medication used to treat ulcers to treat your CML but I would hope that they might.
I am going to continue to take my medication and try the Misoprostol from time to time. I will also be looking to try TFR to see if this truly did work or not but likely will not attempt it until September or later.
Edit: The table feature does not work so had to create an image, store it on my blog and link it here. If you cannot view the image, let me know.






